




TheraP study comparing radioligand treatment with ¹⁷⁷Lu-PSMA to the chemotherapy using cabazitaxel
Findings
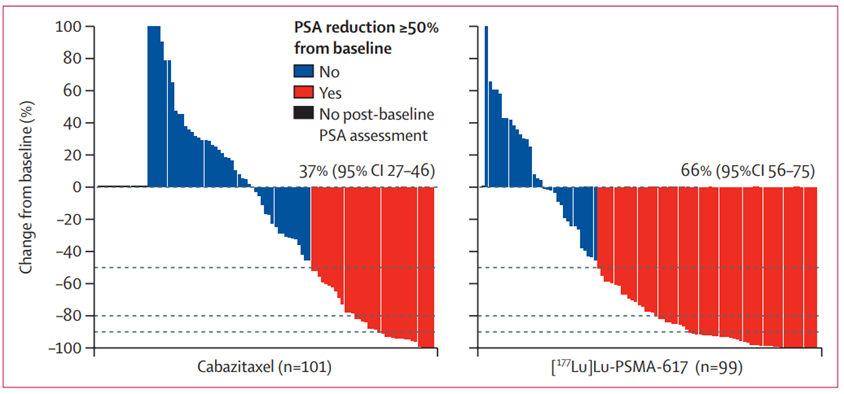
| The primary endpoint or the main success criterion was defined as PSA decline above 50% from the starting values. 177Lu-PSMA-617 compared with cabazitaxel led to a higher PSA response and fewer grade 3 or 4 adverse events.
PSA decline of over 50% was more frequent among those treated with the ¹⁷⁷Lu-PSMA-617 than in the cabazitaxel group: 65 vs 37 PSA responses or 66% vs 44%. Moreover, the higher the SUV was, the better were the odds of the therapy being effective, even with more aggressive tumors (Metabolically active Tumor Volume > 200ml). |
 |
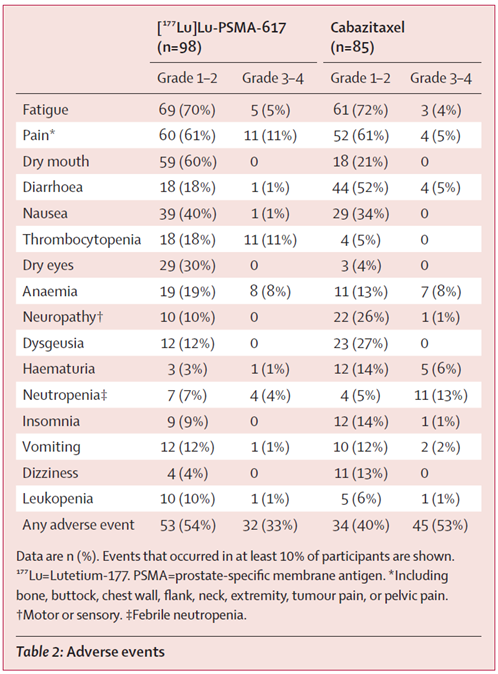 |
Grade 3–4 adverse events occurred in 32 (33%) of 98 men in the 177Lu-PSMA-617 group versus 45 (53%) of 85 men in the cabazitaxel group. |
| 177Lu-PSMA-617 delayed progression as compared with cabazitaxel. Progression-free survival was defined as the interval from randomisation to first evidence of PSA progression defined by an increase of at least 25% and at least 2 ng/mL after 12 weeks. | 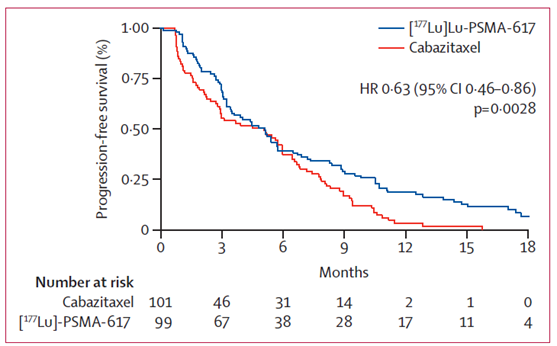 |
